Parathyroid Surgery
Parathyroid surgery, medically known as parathyroidectomy, is a specialized procedure designed to treat disorders of the parathyroid glands.
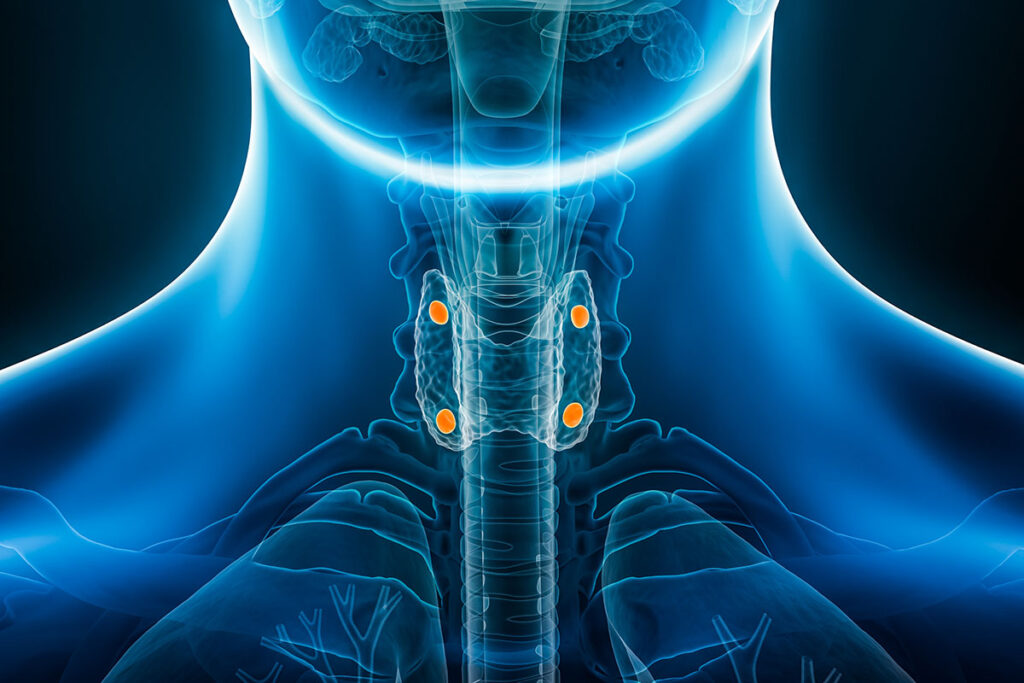
These small, pea-sized glands are located in the neck, adjacent to the thyroid gland, and play a crucial role in regulating calcium levels within the body. Parathyroid surgery becomes necessary when one or more of these glands become overactive, leading to a condition called hyperparathyroidism.
About hyperparathyroidism
The parathyroid glands are 4 small glands in the neck that lie behind the thyroid gland. They are directly adjacent to and sometimes attached to the thyroid. They control the amount of calcium in the blood by secreting parathyroid hormone (PTH). As your body detects that the calcium level is low, more hormones are released and the calcium is raised by several mechanisms.
Primary hyperparathyroidism
The most common disorder of the parathyroid glands is overproduction of parathyroid hormone. This is usually due to one of the four glands developing an adenoma, a benign tumor that does not respond to normal signals to stop secreting hormones. As the parathyroid hormone level rises, so does the serum calcium level. This is called primary hyperparathyroidism and is the most common cause of high calcium in the blood in patients that are not in the hospital.
Secondary hyperparathyroidism
Secondary hyperparathyroidism is usually caused by chronic kidney disease and is much less common.
Symptoms
Symptoms of hyperparathyroidism include, “bones, stones, groans, and psychiatric overtones.” That is, achy bones, kidney stones, abdominal discomfort, and mood disorder.
Unfortunately, it is complicated, and symptoms are vague and nonspecific. Most patients are asymptomatic and found with routine lab tests done during a routine health maintenance exam. If repeat blood tests show high calcium again, a parathyroid hormone level (PTH) is often checked. If this is found to be high, the next step should be a consultation with an endocrinologist or parathyroid surgeon. The disorder can also be found with a workup for kidney stones.
The hardest thing to pin on the high calcium and PTH is depression. Depression is a very common disorder and very few cases are related to hyperparathyroidism. Many people do not feel depressed, but after they are treated for hyperparathyroidism, their mood may improve. The depression may not fully improve, but may be easier to treat with lower dosages of antidepressants. High blood pressure may also be worsened.

Testing
Testing includes repeat calcium checks, repeat PTH levels, 24 hour urine calcium testing, ultrasound of the neck and a nuclear medicine scan called a sestamibi scan. The ultrasound and sestamibi scan are used to try to localize the location of a parathyroid adenoma. These may fail to find the cause of the hyperparathyroidism if the problem is due to gland hyperplasia (all 4 glands are enlarged and over secreting) or a possible double adenoma.
For those that cannot be localized, new protocols for CT scans have been shown to be successful. Dexa scans measure the bone density. This is important, because hyperparathyroidism keeps calcium from being deposited in bones, increasing the risk of osteopenia and osteoporosis.
Surgery Overview
Surgery Guidelines
Indications for surgery follow a set of guidelines. There is some controversy surrounding the need for surgery in people, who are asymptomatic. Studies have shown that if hyperparathyroidism is not treated, most will eventually develop symptoms. Reasons for surgery are age less than 50, serum calcium greater than 1.0 mg/dl above normal, decreased kidney function and signs of osteoporosis, or if medical surveillance is impossible or not desired.
Reasons for surgery are:
- Age less than 50
- Kidney stones
- Osteoporosis
- Serum calcium 1.0 mg/dl above normal
- Decreased kidney function,
- 24 hour urine calcium level greater than 400
About the Surgery
The mainstay of treatment is surgery. The FDA has approved the use of a drug called Sensapar that may help lower calcium levels and is usually used in patients, who are not good candidates for surgery. Surgery includes general anesthesia and a small incision in the front of the neck, going behind the thyroid and directing the search to the area defined by the ultrasound and sestamibi scan or the special CT. About 90% of the time, a single adenoma is found and the surgery is successful.
The locations of the glands are not constant and if the imaging scans are not definitive, the search for the offending gland can be tedious and may take several hours. Occasionally, a parathyroid gland may be inside the thyroid gland, requiring the removal of half of the thyroid. Some techniques have been tried to aid in the locating of the adenoma, such as nuclear medicine guided surgery.
Successful surgery can be confirmed in the operating room with getting rapid PTH assays to measure the levels of PTH in the blood after removal of the gland. PTH drops quickly; once the tumor is removed, the surgical team has to sit, wait, and not manipulate the neck for 10 minutes. The levels are redrawn and compared to earlier test to see if they have dropped enough, indicating successful surgery. Newer technologies have introduced robotic surgery to the armamentarium of some surgeons. Many hope that this will lead to better tolerance of the procedure with less side effects for the patient. The incision in the armpit is well hidden, but definitely not minimally invasive, since the distance needed to reach the neck is much longer. There is no proven improvement in safety or complication rates and the costs of surgery both in expensive equipment and time spent in the operating room are increased.
Surgery Risks
Risks of surgery include bleeding and infection as with any surgery, hoarseness due to damage to the nerve to the voice box, failed surgery (persistent hyperparathyroidism and high calcium after surgery), scar at the incision site, low parathyroid hormone and low calcium, and risks of general anesthesia.
Radio Frequency Ablation
Radio frequency ablation, or RFA, is a minimally invasive procedure used to shrink thyroid nodules. A needle shaped electrode is guided into the nodule using ultrasound. The electrode is then activated while it is in the nodule. Unlike traditional surgery, which involves removing the nodule with a scalpel, RFA utilizes radio waves to generate heat. The electrode is moved through the nodule to treat the whole area. This heat disrupts and destroys the targeted tissue within the nodule, causing it to shrink over time. The surrounding healthy thyroid tissue remains unaffected.
Request an Appointment
Same and next day appointments available